SNAP Is Linked With Improved Health Outcomes and Lower Health Care Costs
A substantial body of research links the Supplemental Nutrition Assistance Program (SNAP), the nation’s most important anti-hunger program, with lower health care costs and improved health outcomes. Those include better self-reported health, lower risk of heart disease and obesity among adults who had access to SNAP as children, and greater medication adherence among older participants, who may also be better positioned to live on their own in their community. This research has emerged in the last 15 years (and not much of it yet reflecting the COVID-19 pandemic, during which SNAP expansions played a key part in averting increased hunger), adding to previous work showing SNAP’s powerful capacity to help families buy adequate food, reduce poverty, and help stabilize the economy during recessions.
SNAP (formerly food stamps) is the primary source of nutrition assistance for many low-income people. In a typical month of 2021, SNAP helped about 41.5 million low-income Americans afford a nutritious diet. It provides important nutritional support for low-paid working families, older adults with low incomes, and people with disabilities living on fixed incomes. Two-thirds of SNAP participants are in families with children, and over a third are in households with older adults or people with disabilities. SNAP provides an estimated $183 a month (or about $6.10 a day) per person in regular SNAP benefits in fiscal year 2023. This modest benefit nevertheless forms a critical foundation for the health and well-being of low-income people, lifts millions above the poverty line, and improves people’s food security, allowing them to spend more on nutritious food than their limited budgets would otherwise allow.[2]
Pinpointing SNAP’s impact presents a daunting challenge in part because it is so widely available and because participants tend to be substantially different from non-participants (for example, participants may have greater unmet food needs or face additional barriers to accessing food). Research emerging in the last 15 years suggests that SNAP may affect household well-being in ways that extend beyond its intended aim to improve food security and nutrition. The available evidence consistently indicates that SNAP is associated with and likely promotes better health and lowers health care costs.
It is therefore plausible that policies that expand program eligibility and raise SNAP benefits would improve health and reduce health care costs while policies that limit eligibility and cut benefits would harm health and raise health care costs. Substantial research on SNAP and related areas has shown:
- Food insecurity increases the risk of adverse health outcomes, complicates the ability to manage illness, and is linked to higher health care costs. On average, after controlling for a range of socioeconomic and demographic characteristics expected to affect food security and health care costs, people in food-insecure households — those lacking consistent access to adequate food at some point during the year due to limited resources — spend roughly 45 percent more on medical care in a year ($6,100) than people in food-secure households ($4,200). And extensive research has shown a strong correlation between food insecurity and chronic health conditions among various age groups: children, young and working-age adults, and older adults.
- SNAP improves food security, offers benefits that enable families to purchase healthier diets, and frees up resources that can be used for health-promoting activities and needed medical care. SNAP reduces the overall prevalence of food insecurity by as much as 30 percent, and is even more effective among children and those with “very low food security,” that is, when one or more household members have to skip meals or otherwise eat less during the year due to lack of money. The largest and most rigorous examination of the relationship between SNAP participation and food security found that food insecurity among children fell by roughly a third after their families received SNAP benefits for six months.
- SNAP is associated with improved current and long-term health. SNAP participants are more likely to report excellent or very good health than low-income non-participants. Early access to SNAP among pregnant mothers and in early childhood improved birth outcomes and long-term health as adults. Elderly SNAP participants are less likely than similar non-participants to forgo their full prescribed dosage of medicine due to cost. SNAP may also help low-income older adults live independently in their communities and avoid hospitalization.
- SNAP is linked with better access to preventive health care and reduced health care costs. Infants and children in families participating in SNAP are more likely to see a doctor for periodic check-ups. Low-income adults participating in SNAP incur an average of about $1,400, or nearly 25 percent, less in medical care costs in a year than low-income non-participants. The difference is even greater for those with hypertension (nearly $2,700 less) and coronary heart disease (over $4,100 less).
SNAP is an effective program that helps millions of people in the U.S. access a nutritious diet, but there’s room to build upon its successes. Ensuring that benefits are adequate, extending eligibility to certain individuals who are ineligible now and eliminating administrative barriers to participation for eligible participants would make SNAP even stronger. Congress took a major step toward benefit adequacy in the bipartisan 2018 farm bill, in which it directed USDA to update the Thrifty Food Plan (TFP) to more accurately reflect the cost of a healthy diet. USDA in August 2021 completed this science-based revision to the TFP, which is used to set SNAP benefit levels, resulting in a 21 percent increase in maximum SNAP benefits effective October 2021. This helped address a situation where many households were running out of benefits before month’s end and where a large body of research found that existing SNAP benefits were well short of what households needed to ensure a healthy diet. Congress should protect SNAP’s ability to help people afford a healthy diet and reduce their risk of food insecurity and poverty.
Policymakers could also take the opportunity in the 2023 farm bill to strengthen SNAP by ensuring it can help all who need it. Some groups who need assistance are ineligible for SNAP, including some adults who face a three-month time limit, several groups of lawfully present immigrants, and formerly incarcerated individuals with drug felony convictions. Many others who are eligible face barriers to applying or staying connected to the program. Puerto Rico, American Samoa, and the Commonwealth of the Northern Mariana Islands have inadequate, capped annual block grants for food assistance that, unlike SNAP, can’t expand to provide benefits for the growing number of eligible beneficiaries during slow economic times.
The Importance of Social Determinants of Health
Research accumulated over the last few decades has firmly established the powerful effects of the circumstances in which people grow, live, work, and age on health, development, and longevity.[3] People disadvantaged by poor social and economic circumstances and neighborhood environments — including low income, poor education and housing, insecure employment, and inadequate retirement pensions — have worse health from the moment of birth throughout life. Economic inequality, for example, is linked to disparities in life expectancy and multiple indicators of good health. An average 40-year-old in the poorest 1 percent of men in the U.S. is expected to die 15 years sooner on average than a man in the richest 1 percent; the gap for women in the U.S. is ten years.[4] Poor adults are five times as likely as those with incomes above 400 percent of the federal poverty level to report poor or fair health. People with low incomes have higher rates of physical limitations, heart disease, diabetes, stroke, and other chronic conditions compared to people with higher incomes. These disparities emerge early in life and can be transmitted across generations.[5] And research suggests that patients in disadvantaged neighborhoods have poorer health care outcomes, more frequent use of emergency rooms, increased risk of hospitalization, delays in diagnosis and treatment, and more difficulty adhering to medication regimes.[6]
Race and ethnicity strongly influence both socioeconomic status and health outcomes. Extensive research shows that people of color have less access to health care, receive a lower quality of care, and have higher rates of chronic disease and death than white people. They are less likely than white people to have health insurance, have more difficulty getting health care, and have fewer choices of where to receive care. They tend to experience lower quality of care and are less likely to receive even routine medical procedures, even after adjusting for socioeconomic differences and other factors that might affect access to health care.[7] There are many reasons for these racial health disparities, but the literature suggests that a central role is played by chronic financial hardship caused by centuries of exploitation and segregation, as well as the direct toxic effects of discrimination on mental and physical health.
The onset of the COVID-19 pandemic magnified existing health disparities for marginalized populations. While the impacts of the pandemic and its economic fallout have been widespread, people of color have borne a disproportionate burden, with higher rates of infection, hospitalization, and death.[8] These disproportionate impacts reflect harsh, long-standing inequities in education, employment, housing, and health care that the crisis exacerbated.
While the ways that social and economic circumstances affect health are complicated and not fully understood, some research implicates repeated or chronic stress — including that stemming from financial and economic hardships — in the more rapid onset or progression of chronic illnesses. The communities in which many low-income people live have higher levels of violence, discrimination, and material deprivation, and many families face multiple challenges, including unstable income, inadequate housing, insecure employment, and poor mental and physical health.[9] The accumulated strain from trying to meet basic needs for food, shelter, and clothing when money is tight may lead to more damage than a single dramatically stressful event.[10]
Food insecurity — when access to adequate food is limited by income — may affect health through multiple channels, including budget constraints that limit access to healthy food choices, the prioritization of food purchases over health care needs such as prescription refills or preventive care, and as a component of overall family stress. Families that struggle with limited resources to put enough food on the table may buy more affordable but less nutritious foods. And the anxiety associated with unpredictable or intermittent meals may be a source of chronic stress that, if left unchecked, can contribute to an increased risk of chronic conditions, including high blood pressure, heart disease, obesity, and diabetes.
Food assistance programs like SNAP can help prevent or moderate the effects of food insecurity. Though its benefits are modest, SNAP helps low-income individuals and families who struggle to afford basic needs have enough to eat, enables them to afford healthier diets, and frees up resources that can be used on health-promoting activities and preventive health care. The benefits it provides may also offset some of the stress associated with food insecurity and make it somewhat easier to manage chronic illness. Thus, SNAP may offer a pathway to improved health and lower public expenditures on health care.
Food Insecurity Is Associated With Poor Health Outcomes
Extensive research reveals a consistent and strong correlation between food insecurity and poor health outcomes across a person’s life cycle:[11]
- Among children, food insecurity is linked to increased risks of poor health, poorer diet quality, development of chronic health conditions including asthma and anemia, cognitive and behavioral problems, and anxiety and depression.[12]
- Among young adults, food insecurity is linked to increased risks of poor health, chronic health conditions including diabetes, asthma, bronchitis, emphysema, and hypertension, and unhealthy weight.[13]
- Among working-age adults, food insecurity is linked to increased risks of poor general and mental health, poorer diet quality, and chronic health conditions including hypertension, coronary heart disease, diabetes, and kidney disease.[14]
- Among older adults, food insecurity is linked to poor health and depression, poorer diet quality, chronic health conditions including diabetes and anemia, more limitations in daily activities, and decreased quality of life.[15]
Research suggests that even marginal food security and episodic food insecurity may lead to adverse health outcomes, although the strength of association is weaker than that for food insecurity (low or very low food security). Marginal food security, defined by at least one reported indication of stress related to having insufficient food (but not as many indications as those considered food insecure), has been linked with increased health and developmental risks in young children and poorer health among their caregivers.[16] Parental reports of their child’s health are also worse in households that transition from food security to food insecurity compared to those who remain persistently food secure.[17]

Researchers at the U.S. Department of Agriculture’s (USDA) Economic Research Service documented the strong correlation between food insecurity and chronic health conditions among low-income working-age adults. Their work shows that the risk of each of ten chronic conditions — hypertension, coronary heart disease, hepatitis, stroke, cancer, asthma, diabetes, arthritis, chronic obstructive pulmonary disease, and kidney disease — increases substantially as the severity of food insecurity increases (see Figure 1). Adults in households with very low food security are at least 40 percent more likely to be diagnosed with at least one of the ten chronic diseases than adults in highly food-secure households.[18]
The health risks and hardship associated with food insecurity fall disproportionately on people of color. Over the past 20 years, both Black and Hispanic households have been at least twice as likely as white households to experience food insecurity (see Figure 2). In 2021, 19.8 percent of Black households experienced food insecurity, as did 16.2 percent of Hispanic households, compared to 7.0 percent of white households.[19] And food insecurity among households headed by Black adults worsened between 2019 and 2020 at the onset of the pandemic even as overall levels of remained unchanged due to a robust relief effort.

While existing research has established a strong association between food insecurity and physical and mental health, the evidence that food insecurity causes poor health outcomes is more limited but highly suggestive. Some researchers have used quasi-experimental methods to compare outcomes among children who differ in their food security status but are otherwise similar, with results pointing to pervasive harm by household food insecurity on children’s health: children in food-insecure households are two to three times more likely to delay or forgo needed medical, dental, and mental health care because of its costs; more likely to visit an emergency room; and at higher risk for asthma. Other researchers estimated boundaries on the potential size of causal effects of food security on children’s health outcomes while accounting for the uncertainty created by unobserved differences and potential errors in the measurement of food security status. They conclude that food security has a statistically significant positive impact on general health and healthy weight and suggest that previous research has more likely underestimated than overestimated the causal impacts of food insecurity on health.[20]
Despite this recent progress, much of the existing research is based on study designs that make it difficult to determine conclusively the extent to which food insecurity causes poor health, poor health contributes to food insecurity, or other unobserved factors contribute to both. Food insecurity may cause poor health through limited budgets, which may force families to purchase cheaper but less healthy food, or make a choice between buying food or medications, with adverse consequences for their health. Stress, fatigue, or depression may occur during episodes of food insecurity, negatively impacting health. Conversely, poor physical or mental health may make it harder to work, for example, leading to lower income and increasing the risk of food insecurity. But regardless of the precise mechanism that links the two, food insecurity is a strong predictor of poorer physical and mental health.
Food Insecurity Is Associated With Cost-Related Medication Underuse
People facing food insecurity may put off attending to their health when faced with other pressing needs, choosing food over medication, postponing needed medical care, or forgoing special medical diets, for example. Skipping some or all medication due to cost is a significant public health problem that affects the health and well-being of as many as 1 in 4 working-age adults.[21]
Several studies based on large national surveys find that food insecurity is associated with the underuse of medication due to cost among working-age adults, including those with chronic disease and diabetes, and among older adults.[22] Among working-age adults, for example, those in food-insecure households are about four times more likely to have a problem with medication underuse because of cost than those in food-secure households, even after adjusting for differences in the characteristics of food-secure and food-insecure households. There is also evidence that cost-related medication underuse increases with the severity of food insecurity: compared to people in food-secure households, for example, people in households with marginal food security are about 50 percent more likely to have at least one cost-related medication problem, people in households with low food security are more than twice as likely, and those in households with very low food security, the most severe form, are more than three times as likely (see Figure 3).[23]

Among people of color, inability to afford prescription medication is of particular concern since they are more likely to be food insecure and chronically ill. Average adherence rates of Black and Hispanic patients were about 5 to 7 percentage points lower than white patients across three widely used drug classes in one recent study, which translates to about 20 to 25 fewer days of medication use per year, even after adjusting for other differences in socioeconomic characteristics.[24]
Food Insecurity Is Associated With Higher Health Care Use and Costs
Food insecurity imposes a substantial burden on society, including lost productivity and avoidable health care costs. Those who experience food insecurity tend to make greater use of and spend more on health care than those who are food secure. While it may not be possible to create a precise estimate of food insecurity’s economic burden, there is reason to think it could be substantial.[25]
Canadian researchers, for example, using linked survey and administrative data on 67,000 working-age adults in Ontario province, show that public health care expenditures are substantially higher for food-insecure people, even after adjusting for other socioeconomic and demographic characteristics that might affect either food security or costs. The findings are particularly compelling because the study occurred in the context of Canada’s universal health care system, meaning it is unlikely that observed differences are due to differences in access to health insurance. The researchers found that individuals in households with moderate food insecurity are a third more likely to use health care services — and expenses among these health care users are a third higher — than those in food-secure households. And as food insecurity increases, so do health care costs. People in households with the most severe food insecurity are 71 percent more likely to use health care services, and the expenses of these health care users are 76 percent higher, than those in food-secure households. (See Figure 4.)[26]

A recent analysis of national survey data representing virtually all of the Canadian population aged 12 and older found results broadly consistent with the Ontario study. The severity of food insecurity was associated with a greater likelihood of being hospitalized, higher odds of readmission, longer stays, and higher expenditures once hospitalized. Individuals in households with moderate food insecurity were 40 percent more likely to be admitted to a hospital, and expenses among these health care users were 42 percent higher, than those in food-secure households. People in households with the most severe food insecurity were 69 percent more likely to be admitted and had expenses that were 44 percent higher.[27]
Researchers in the United States, using national survey data to capture out-of-pocket expenses and insurance payments for two years after a household experiences food insecurity, found similar results. On average, again after adjusting for a range of socioeconomic and demographic characteristics expected to affect food security and spending on health care (both out of pocket and paid by insurance, including Medicare and Medicaid), people in food-insecure households spend roughly 45 percent (or $1,900) more on medical costs in a year ($6,100) than people in food-secure households ($4,200). The increase in expenditures is most pronounced for people with chronic conditions: annual health care costs are $4,400 higher among those with diabetes, $2,200 higher among those with hypertension, and $5,100 higher among those with heart disease.[28] The odds of becoming a high-cost health care user in the future are 46 percent greater for food-insecure people than for those who are food secure.[29]

While these results do not on their own fully establish a causal relationship, the study’s longitudinal design provides evidence that exposure to food insecurity is likely associated with higher health care expenditures.[30] This association could work in one of two directions. Food insecurity could be a cause of poor health and thus higher health care expenditures. But poor health and higher health care expenditures could lead to food insecurity by impeding the ability to work or diverting resources needed for food toward medical expenses. Recent research that compared food security in one year to health care expenditures in the following year (and vice versa) found evidence of this bidirectional relationship. But, while higher health care expenditures were associated with a slightly greater risk of being food insecure, being food insecure was associated with substantially greater health care expenditures. Each $1,000 difference in health care spending increased the risk of food insecurity by about 1 percent; health care expenditures of food-insecure people, however, were about 25 percent ($1,700) more than for those who were food secure.[31]
Food insecurity is also associated with greater use of health care services. Children living in households with food insecurity are more likely to have no usual source of care, postpone medical care and medications, and visit an emergency room. Their parents are more likely to experience difficulty when accessing health care services, as they prioritize competing basic needs and choose to allocate limited resources to food or housing before health care.[32] Adults in food-insecure households are about 50 percent more likely to visit an emergency room and to be admitted to a hospital, and they stay hospitalized about 50 percent longer, than adults in food-secure households (see Figure 5).[33] Older people who are food insecure are also more likely to make use of health care services, including office visits, overnight stays in a hospital, and emergency rooms.[34]
SNAP Helps Put Food on the Table and Improves Food Security

SNAP serves a vital role in improving the well-being of low-income people by making adequate, nutritious food more affordable. Because SNAP enables low-income households to spend more on food than their limited budgets would otherwise allow, it makes it easier to put enough food on the table.
Estimating SNAP’s impact on food security is challenging, however, because households that participate in SNAP differ in systematic ways from households that do not. Notably, one of the main tools researchers use to separate a program’s impact from such differences — a randomized control trial — is generally not feasible with SNAP because withholding nutrition benefits from a random sample of low-income individuals raises serious ethical questions. (See Appendix II.) Failing to account for those differences can lead to misleading results. It is hard to imagine how, for example, giving a family more resources to buy food could reduce their food security as some early studies suggested. Recent evidence, based on studies with stronger research designs that support causal inferences, shows that SNAP participation does substantially improve food security. SNAP reduces the overall prevalence of food insecurity by as much as 30 percent, and is even more effective among children and those with very low food security.
The largest and most rigorous examination of the relationship between SNAP participation and food security found that overall food insecurity fell by as much as one-fifth and that food insecurity among children fell by roughly a third after their families received SNAP benefits for six months (see Figure 6).[35] Researchers at the Urban Institute used national survey data from the late 1990s and early to mid-2000s to show that SNAP reduces the likelihood of being food insecure by roughly 30 percent and the likelihood of being very food insecure by roughly 20 percent.[36] Other researchers more recently concluded that SNAP participation reduces the probability of food insecurity among children by more than 20 percent.[37] SNAP may be especially effective helping those with the greatest need: among households most likely to be the most food insecure, participating in SNAP reduced the probability of food insecurity by almost half.[38]
There is also direct evidence that a more generous SNAP benefit helps many more families afford adequate food. USDA’s large-scale randomized experiment to test the effects of providing additional benefits during summer months when children do not have access to free or reduced-price school meals produced striking results: the additional benefits reduced very low food security among children by about one-third.[39] These results are especially important given the October 2021 increase in maximum SNAP benefits based on an updated Thrifty Food Plan (TFP). The revised TFP more accurately reflects the cost of a healthy diet and is better aligned with current dietary recommendations and the economic realities most struggling households face when trying to buy and prepare healthy foods. (See Appendix I: Effect of Updated Thrifty Food Plan.)
Crisis-driven relief efforts provide evidence that higher benefits mitigate food insecurity. Food insecurity fell after the American Recovery and Reinvestment Act of 2009 (ARRA) temporarily increased SNAP benefits to help those affected most by the Great Recession.[40] And, while researchers have only just begun assessing the direct impacts of SNAP on food security and health amid the pandemic, SNAP expansions likely played a key part in preventing a rise in overall food insecurity during the unprecedented crisis.[41] These expansions included giving states flexibility to provide emergency SNAP benefit supplements, which all states did; boosting SNAP maximum benefits by 15 percent from January through September 2021; and creating a Pandemic-EBT program to provide benefits (via SNAP EBT cards) to households with children who missed school meals due to the pandemic.
Early evidence shows that receipt of Pandemic-EBT benefits in 2021 reduced the share of SNAP households where children experienced very low food security by 17 percent and reduced food insufficiency among SNAP households by 28 percent.[42] And the number of people reporting they did not have enough to eat fell after maximum benefits were increased 15 percent.[43]
SNAP Is Associated With Improved Current and Long-Term Health Outcomes
Maintaining good health requires ongoing investment of both time and money. It can be difficult for low-income households to make those investments when faced with multiple demands on limited budgets. The food assistance SNAP offers is modest but may nevertheless make it easier for individuals and families to afford healthier food. SNAP benefits also free up resources that can be used on health-promoting activities and preventive health care by reducing what families must spend out of pocket on food. And the addition of SNAP benefits to a household’s budget may reduce the stress associated with not having enough money to feed a family. Some positive health impacts may be seen in the short term, but other potential health benefits may take longer to emerge and depend on how long families participate and the amount of benefits they receive.
While not conclusive, existing research suggests that SNAP may, in fact, offer a pathway to better health.
SNAP is associated with improvements in current health. After adjusting for differences in demographic, socioeconomic, and other characteristics, adults who participate in SNAP are more likely to assess their own health as excellent or very good (see Figure 7), as are parents who assess their child’s health. Adults have fewer sick days, make fewer visits to a doctor, are less likely to forgo needed care because they cannot afford it, and may be less likely to exhibit psychological distress.[44]
Figure 7 Researchers have shown that children receiving SNAP are less likely than low-income non-participants to be in fair or poor health, underweight, or obese, and their families are less likely to make tradeoffs between paying for health care and paying for other basic needs, like food, housing, heating, and electricity.[45] Children who lose some or all of their SNAP benefits are more likely to have poor health and be food insecure compared to children in families that maintain benefits, and families that lose benefits are more likely to forgo medical care or make health care tradeoffs than families who consistently receive SNAP benefits.[46] Another line of research suggests that SNAP may protect against poor cardiometabolic health (characterized by abdominal obesity, lipid imbalances, elevated blood pressure, glucose intolerance and insulin resistance) among youth in low-income families.[47]
Recently published research also suggests that participating in SNAP may prevent poor physical health resulting from food insecurity among older adults. The correlations between very low food security and physical health outcome were negatively significant prior to SNAP enrollment but became insignificant upon participation among people aged 50 and older.[48]


Early access to SNAP can improve birth outcomes and long-term health. Poor nutrition during childhood may harm health and earnings decades later by altering physical development and affecting the ability to learn. Researchers comparing the short- and long-term outcomes of individuals in different areas of the country when SNAP (then the Food Stamp Program) expanded nationwide in the 1960s and early 1970s found that mothers who had access to the program during pregnancy gave birth to fewer low-birth-weight babies. Adults with access to food stamps in early childhood had lower risks of obesity and other conditions related to heart disease and diabetes (see Figure 8).[49]
Research that followed children for nearly 20 years into early adulthood shows that those who experienced very low food security during childhood had worse self-reported health, greater likelihood of chronic conditions, and more hospitalizations in adulthood. Even marginal food security or episodic food insecurity during childhood increased the likelihood that individuals experience psychological distress as young adults.[50]Similarly, the experience of children of immigrants during a period when eligibility rules changed for their parents offers evidence that an additional year of SNAP eligibility in early life (from in utero to age 4) is associated with improvements in health outcomes — parental reports of health status, overnight hospitalizations, and number of doctor’s visits — between ages 6 and 16, providing evidence that participating in the program as a young child can impact later-life health as soon as school age.[51] While immigrants are a select and relatively more disadvantaged group of SNAP participants, children of immigrants account for about a quarter of all children and one-third of children in poverty. Congress eliminated SNAP eligibility for most low-income individuals with lawful immigration status in 1996, but reversed many of these restrictions between 1998 and 2003. These changes in eligibility allow for a relatively strong test of the impact of SNAP on children’s health, as the researchers compared health outcomes among children whose parents lost eligibility for SNAP when they were in early childhood to similar children whose parents remained eligible.
SNAP is associated with better access to preventive health care. Wellness visits, especially in the first year of life, are important for child health. There is some evidence that each additional month of SNAP benefits increases the likelihood that an infant receives the recommended number of well-child visits, perhaps by reducing the need to prioritize immediate food needs over preventive care. Moreover, families who leave SNAP or participate inconsistently are less likely to make all the recommended well-child visits.[52] Families often leave SNAP not because their financial circumstances improve but due to administrative reasons, such as when complex application or renewal processes prevent them from participating. And much like inequities in other areas, Black and Hispanic families are especially less likely to make all recommended well-child visits.
Similarly, families who live in areas with lower food prices — and who, therefore, have a somewhat easier time stretching their SNAP benefits to meet their food needs — may be more likely to take advantage of needed medical care. One study suggests, for example, that children who live in lower-cost areas (with higher SNAP purchasing power) are more likely to have had an annual check-up and may be less likely to delay or go without medical care due to its cost. Children who live in higher-cost areas (with lower SNAP purchasing power) miss more days of school due to illness.[53]
SNAP Is Linked With Improved Medication Adherence

As noted above, people experiencing food insecurity are more likely to put off prescription refills, skip doses, or take less medication than prescribed to save money.[54] Diabetes and hypertension — both among the leading causes of poor health and mortality in the U.S. — are widely prevalent among low-income older adults, including those participating in SNAP. Taking medications to manage these conditions is critical to maintain good health and prevent avoidable complications and hospitalizations.[55] SNAP may help participants adhere to medication regimens by reducing their out-of-pocket costs for food, freeing up resources that might be used for medication.
Few studies have considered — and only two have focused on — SNAP’s impact on cost-related medication underuse. These analyses, of SNAP participants aged 60 and older with diabetes, conclude that they are about 5 percentage points less likely to cut back on their medications because of cost than eligible non-participants, a 30 percent reduction. This difference persists even after controlling for differences in food security between the two groups: even among only those in food-insecure households, older SNAP participants are still 7 percentage points less likely to have cost-related medication problems than eligible non-participants, a reduction of 26 percent. (See Figure 9.)[56] These results suggest that increasing access to SNAP might make it easier for low-income seniors to afford their prescription medications.
SNAP Is Associated With Reduced Health Care Costs
Recognition of the importance of social determinants of health calls attention to programs, policies, and practices that shape the physical and social environments in which individuals live and work. Some of the most important opportunities for improving health and reducing health care spending may be found in economic and social resources that promote healthy living and working conditions and healthy choices. By increasing access to healthier food choices and reducing the stress of food insecurity, as well as by freeing up resources that participants can spend on their health, SNAP may be one such path to lower health care costs.
SNAP is associated with fewer nursing home and hospital admissions, especially among older participants, and less frequent visits to a doctor’s office or emergency room. Researchers looking at over 60,000 low-income seniors in Maryland report that SNAP participants are 23 percent less likely to enter a nursing home and 4 percent less likely to be hospitalized in the year after receiving SNAP than non-participants. The amount of SNAP benefits received also matters: larger monthly benefits were associated with a further reduction in the odds of nursing home admissions, the length of stays among those admitted, and the likelihood of hospitalization (see Figure 10).[57]
This research controls for several socioeconomic and demographic characteristics that could otherwise bias the results. Similarly, it also controls for chronic conditions and Medicaid participation, which would affect health and health care utilization outcomes. Despite this design, it may not fully account for unobserved differences between participants and non-participants. It is noteworthy, however, that analyses using the amount of SNAP benefits received rather than simply participation in the previous year reveals a similar relationship with the likelihood of nursing home and hospital admissions. Because that analysis is limited to those who participate in SNAP and looks only at differences in the amount received, it is not subject to the same concern about self-selection into the program.
Figure 10 Researchers found similar results among older adults eligible for both Medicare and Medicaid in North Carolina. Participation in SNAP was associated with fewer inpatient hospitalizations, emergency room visits, and long-term care admissions as well as lower annual Medicaid payments.[58] There is also some evidence that larger SNAP benefits are associated with a reduction in the number of Medicaid claims for emergency room visits to treat hypertension.[59] One study compared the health care utilization of immigrants who regained SNAP eligibility between 1998 and 2003 to those who remained ineligible and found that SNAP reduced the need for repeated visits to doctors’ offices for primary care, emergency room visits, and hospitalizations among relatively healthy participants.[60]
More generally, research using longitudinal data that followed older adults for ten years suggests that food-insecure seniors who participate in SNAP are 46 percent less likely to be hospitalized than non-participating, low-income seniors. Even among food-secure seniors, participation is associated with an 18 percent reduction in the likelihood of hospitalization.[61]

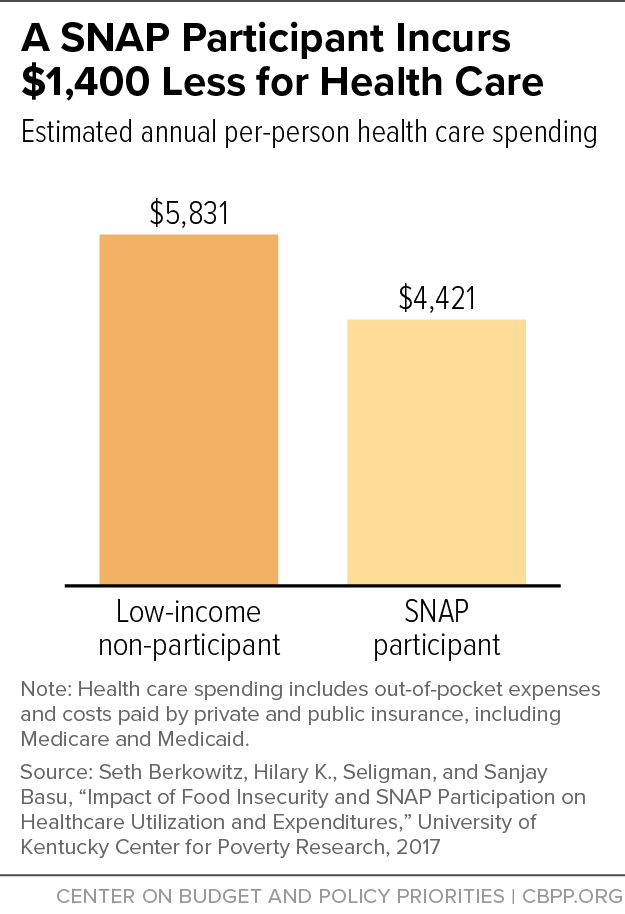
- SNAP participation is also linked with lower overall health care expenditures and Medicaid/Medicare costs. An analysis of national data on overall health care expenditures links SNAP participation to lower health care costs among low-income adults.[62] On average, after controlling for factors expected to affect spending on medical care, adults participating in SNAP incur about $1,400, or nearly 25 percent, less in medical care costs in a year, including those paid by private or public insurance, than non-participants. (See Figure 11.) The differences are even greater among those with hypertension (nearly $2,700 less) and coronary heart disease (about $4,100 less).[63] While the approach used to generate these results may not fully account for unobserved differences between SNAP participants and non-participants, two alternative analyses that mitigate potential for bias due to self-selection into SNAP also demonstrate reduced health care expenditures — of as much as $5,000 — associated with SNAP participation.[64] None of these approaches, however, accounts for either the duration or amount of benefits received.
Conclusion
The research reviewed here suggests that policies to improve the food security of low-income individuals and families and increase their access to SNAP might reverberate across a variety of health outcomes. Food insecurity is strongly associated with increases in the risk of adverse health outcomes, may complicate the ability to manage illness, and is linked to higher health care costs. SNAP improves food security, offers benefits that enable families to purchase healthier diets, and frees up resources that can be used for health-promoting activities and needed medical care. Policies that address food insecurity, SNAP participation, and benefits could improve health, reduce health disparities, and lower costs.
States should be especially interested in the possibility that enrolling low-income eligible individuals and families in SNAP might help reduce health care costs. States and the federal government share the cost of providing health care coverage for low-income individuals and families through Medicaid. The state share of Medicaid costs ranges from about 25 percent to 50 percent, with poorer states paying less.[65] Overall, Medicaid accounts for roughly 15 percent of total state expenditures. In contrast, the federal government is responsible for the entire cost of SNAP benefits.[66] As a result, changes in policies that improve access to SNAP’s benefits could provide short- and long-term relief to state Medicaid budgets.
While the existing evidence has advanced understanding of the relationship between SNAP, food security, and health, important gaps remain. High-quality studies with rigorous designs that adequately address issues of self-selection, underreporting of program participation, and the direction of causation are relatively scarce. Additional investment in future research efforts is needed to:
- Confirm the direction and determine the strength of the causal relationship among 1) food insecurity, SNAP participation, and health status; 2) use of health care services; and 3) health care costs;
- Identify and understand the ways that food insecurity and SNAP participation could lead to changes in health status, use of services, and costs; and
- Determine the extent to which factors such as the duration of exposure to food insecurity or the amount of SNAP benefits received affects health status, use of services, and costs.
Appendix I: Impact of Updated Thrifty Food Plan
On August 16, 2021, the U.S. Department of Agriculture (USDA) announced that it had updated its Thrifty Food Plan (TFP) which is used to set the amount of food assistance for people participating in SNAP. The reevaluated TFP raised maximum SNAP benefits by 21 percent (and average SNAP benefits by 27 percent) in fiscal year 2022 compared to what they otherwise would have been (absent the temporary pandemic relief increases). SNAP households in most states saw a benefit increase as a temporary 15 percent increase ended and the increase in SNAP benefits based on the reevaluated TFP took effect in October 2021. While most SNAP households will see a substantial cut in their SNAP benefits when additional emergency allotments end, their benefits will be higher than they otherwise would have been without the TFP update.
The revised TFP more accurately reflects the cost of a healthy diet and is better aligned with current dietary recommendations and the economic realities most struggling households face when trying to buy and prepare healthy foods. The revised TFP can have a long-term impact on food security, economic mobility, and health.[67]
Although the revised TFP has not been in place long enough for researchers to assess its impact, some important lessons can be drawn from a similar, albeit smaller and temporary, increase in SNAP benefits made in response to the Great Recession. Taking advantage of this natural experiment, researchers found that the temporary increase in SNAP benefits:
- Helped reduce food insecurity and increase people’s spending on food and other essentials. Researchers at USDA’s Economic Research Service, for example, found that food expenditures by low-income households increased by about 5 percent and food insecurity declined by 2 percentage points from 2008 to 2009.[68]
- Improved children’s access to health care. Specifically, children in households eligible for SNAP were less likely to forgo or delay needed medical care and medications because they could not afford it compared to low-income, ineligible children.[69]
- Reduced certain nutrition-related health risks. There is some evidence that ARRA’s increase in SNAP benefits was associated with healthier weight outcomes among low-income youth.[70] Other researchers found evidence of improvements in hemoglobin A1c and total cholesterol levels (important markers of cardiometabolic risk for diabetes or lipid disorders) among young and middle-aged adults eligible for SNAP.[71]
- Slowed growth of Medicaid costs, especially among people with chronic illnesses. By one estimate, Medicaid cost savings amounted to $26.5 billion over the 55 months of increased SNAP benefits.[72]
One of the paths through which SNAP may improve health is through more healthful eating habits. In theory, a household’s participation in SNAP can affect their food choices, diet quality, and nutritional intake by increasing the resources available to purchase food; by enabling households to substitute healthier, possibly more expensive, food for less healthy but cheaper food; or by promoting healthier choices through nutrition education. Decisions about what we eat, however, are guided by many factors, including by biological, economic, physical, social, and psychological determinants, and by attitudes, beliefs, and knowledge about food. Many SNAP participants, like people in the U.S., have diets that fall short of current dietary recommendations.[73] Participants and non-participants, regardless of income, tend to make broadly similar food purchase and consumption choices.[74]
While there is little evidence that SNAP, as historically structured, has had a substantial impact on food choices, diet quality, and nutrient intakes, the variability in study designs, methodology, reference populations, and outcome measures makes it difficult to make meaningful comparisons and draw firm conclusions. In general, research on the relationship between income and diet quality, and the effect of benefit increases on diet quality, has been mixed. [75] For example, the natural experiment offered by the ARRA SNAP benefit increase did not reveal consistent improvements in nutrient intake and diet quality.[76]
But other research using alternative methods to estimate the impact of a benefit increase on diet quality suggests raising SNAP benefits could increase low-income households’ spending on food and also improve the nutritional quality of their diets. Economists simulating an increase in SNAP benefits (equivalent to the recent TFP revision’s 27 percent increase in average benefits) found that it increased food spending (with larger increases for food prepared at home compared to food prepared away from home). The benefit increase also resulted in small but statistically significant improvements to the nutritional quality of food purchases (both overall diet quality and for some components of a healthy diet, such as the relative amount of whole fruit); and increased quantities of several key nutrients, such as iron and calcium.[77]
Appendix II: Evaluating the Causal Impact of SNAP
The modern form of SNAP (formerly the Food Stamp Program) has been a widely available and well-established part of the nation’s safety net for low-income Americans for 50 years. Key features of the program — including a funding structure that makes benefits available to anyone who qualifies under the program’s rules without restrictions to certain categories of low-income individuals — are critical to its success. These same features make the task of evaluating its impacts more difficult.
The gold standard for evaluating the effectiveness of a program or intervention is the randomized control trial, which is designed to minimize the risk that factors unrelated to the program influence the results. If people are randomly assigned to a program, researchers can accurately estimate its impact as the difference in outcomes between those who participate and those who do not because they were randomly selected from the same population, lived through the same shifting programmatic, economic, and social conditions, and differ only in their program experience. However, randomized control trials are generally not feasible to evaluate SNAP’s effectiveness, in part because the program is so widely available, and because withholding nutrition benefits from a random sample of low-income individuals would raise serious ethical questions.
As a result, estimating the effect of SNAP on health, health care utilization, and costs presents a daunting challenge. In addition to disentangling and isolating SNAP participation and benefits from the complex interactions of other social and economic factors, the physical environment, and individual behaviors that determine health, researchers must wrestle with three thorny issues: selection bias, measurement error, and causation.
Selection Bias. In the absence of a randomized control trial, research results may be biased by the self-selection of low-income individuals and families into SNAP. Households that participate in SNAP may differ in systematic ways from households that do not. If those who choose to enroll in SNAP are more motivated, healthier, or have access to better health care than those who do not, then selection bias may lead researchers to mistakenly conclude that SNAP is more effective than it really is. But if those who enroll in SNAP are more disadvantaged, more food insecure, less healthy, or exhibit more risky behaviors than those who do not, then selection bias may lead to conclusions that SNAP is less effective than it really is. Most analyses routinely control for some potential differences, but others — local attitudes toward health and program participation, for example — are usually unobserved and not measured.
The research studies reviewed here have used a variety of data sources and empirical methods, some more rigorous than others, to isolate SNAP’s impact on food insecurity and health from differences in the characteristics of participants and non-participants. There is little reason to put too much confidence in the results of any single study. The consistency of results across studies, however, adds considerable weight to the validity of their collective conclusion that SNAP improves food security.
In addition, most of the available evidence suggests that selection bias is more likely to lead to underestimates of SNAP’s beneficial impacts because participants are more disadvantaged and prone to adverse health outcomes than non-participants. National survey data show that SNAP participants are much less likely to be in excellent or very good health; more likely to be disabled or have a family member with functional limitations; more likely to be diagnosed with attention deficit disorder, asthma, diabetes, back problems, stroke, heart attack, and ulcer; and much more likely to have contact with the medical system but less likely to be able to afford care. When compared to low-income non-participants, SNAP participants are more likely to report worse health, more sick days, and greater use of health care before entering the program than non-participants. SNAP participants are also about a third more likely to die from any cause than low-income non-participants.[78]
Measurement Error. A second issue arises because SNAP participation is underreported in most household surveys. As many as half of SNAP participants fail to report their participation in the program in large-scale national surveys, while few mistakenly report participating when they do not. Even administrative data — often considered the “gold standard” when measuring program participation — are not immune to error (or at least ambiguity).[79] An example illustrates why this matters. Imagine that we can correctly identify a group of 1,000 people eligible for SNAP. Among this group, we know that 800 receive SNAP benefits and 200 do not, consistent with current estimates of SNAP participation rates. We then survey each of them and ask whether they receive SNAP. If half of those who truly participate mistakenly report that they do not, we would count only 400 participants (assuming none of those who did not participate mistakenly report that they did). The other 400 would appear in the survey to be non-participants. Thus, there would be twice as many participants as non-participants in the comparison group of “non-participants,” effectively masking any impact SNAP participation might have on outcomes of interest. Few research studies, and none included in this review, have attempted to account for the measurement error introduced by underreporting of program participation.[80]
Causation. An extensive body of research reveals a strong correlation between food insecurity, and to a lesser extent SNAP, and health. With few exceptions, however, much of this research is based on study designs that make it difficult to determine causation. Ideally, we would like to know whether food insecurity causes poor health, whether poor health leads to food insecurity, or whether there are unobserved factors that jointly influence both food insecurity and health. It is hard to draw definitive conclusions about SNAP’s impact on health through its positive impact on food security absent a strongly established causal link from food insecurity to health.
End Notes
[1] Steven Carlson is a research analyst who previously directed the Office of Policy Support at the Agriculture Department’s Food and Nutrition Service. The opinions and conclusions expressed in this report are solely those of the authors and should not be construed as representing the views of the Agriculture Department.
[2] Estimated fiscal year 2023 benefits exclude temporary, pandemic-related increases and are based on a CBPP analysis of fiscal year 2019 SNAP household characteristics data. They reflect the U.S. Department of Agriculture’s (USDA) recent revision to the Thrifty Food Plan, which is used to set the amount of food assistance that households participating in SNAP receive. See Appendix I, Impact of Updated Thrifty Food Plan.
[3] Paula Braveman, Susan Egerter, and David R. Williams, “The Social Determinants of Health: Coming of Age,” Annual Review of Public Health, 32: 381-98, 2011, http://www.annualreviews.org/doi/pdf/10.1146/annurev-publhealth-031210-101218; Nancy E. Adler et al., “Addressing Social Determinants of Health and Health Disparities,” Vital Directions for Health and Health Care Series, National Academy of Medicine, September 19, 2016, https://nam.edu/wp-content/uploads/2016/09/Addressing-Social-Determinants-of-Health-and-Health-Disparities.pdf.
[4] Raj Chetty et al., “The Association Between Income and Life Expectancy in the United States, 2001-2014,” Journal of the American Medical Association, 315(16): 1750-1766, 2016.
[5] Dhruv Khullar and Dave A. Chokshi, “Health, Income, & Poverty: Where We Are & What Could Help,” Health Affairs Policy Brief, October 2018, https://www.healthaffairs.org/do/10.1377/hpb20180817.901935/full/HPB_2017_RWJF_05_W.pdf.
[6] Andrew Knighton, Brad Stephenson, and Lucy Savitz, “Measuring the Effect of Social Determinants on Patient Outcomes: A Systematic Literature Review,” Journal of Health Care for the Poor and Underserved, 29(1): 81-106, 2018 https://muse.jhu.edu/article/686956/summary.
[7] Brian Smedley, Adrienne Stith, and Alan Nelson, eds., Unequal Treatment: Confronting Racial and Ethnic Disparities in Health Care, National Academy Press, 2003, https://www.ncbi.nlm.nih.gov/books/NBK220358/.
[8] See, for example, William Mude et al., “Racial disparities in COVID-19 Pandemic Cases, Hospitalisations, and Deaths: A Systematic Review and Meta-analysis,” Journal of Global Health, 11: 05015, 2021, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8248751/.
[9] See, for example, Ozge Bahar et al., “‘Like, What Else Could Go Wrong?’ Multiple Contextual Stressors in Food Insecure Households,” Journal of Poverty, 25(4): 386-407, 2021, https://www.tandfonline.com/doi/abs/10.1080/10875549.2020.1840485; and Angela Odoms-Young, “Structural and Social Adversity and Food Insecurity in Families with Young Children: A Qualitative Metasynthesis,” in Families, Food, and Parenting, 2021, https://link.springer.com/chapter/10.1007/978-3-030-56458-2_1.
[10] Richard Wilkinson and Michael Marmot, “Social Determinants of Health: The Solid Facts,” World Health Organization, 2003 (2nd edition), http://www.euro.who.int/__data/assets/pdf_file/0005/98438/e81384.pdf. There is some suggestive, if not conclusive, evidence of the cumulative effect of multiple adverse experiences (such as loss of a parent through separation, divorce, or incarceration; witnessing neighborhood violence; or exposure to alcohol or drug abuse) in early childhood on food insecurity. While young children exposed to a single experience are about twice as likely to experience food insecurity, those exposed to more than one are about four times as likely. See Philip Baiden et al., “Adverse Childhood Experiences and Household Food Insecurity Among Children Aged 0–5 Years in the USA,” Public Health Nutrition, 24(8): 2123-2131, 2021, https://www.cambridge.org/core/journals/public-health-nutrition/article/adverse-childhood-experiences-and-household-food-insecurity-among-children-aged-05-years-in-the-usa/D7E980439685D1FB2ACA0D881FE1384E.
[11] For summaries of the extensive research on the health consequences of food insecurity, see Barbara A. Laraia, “Food Insecurity and Chronic Disease,” Advances in Nutrition: An International Review Journal, 4(2): 203-212, 2013, http://advances.nutrition.org/content/4/2/203.full; Craig Gundersen and James Ziliak, “Food Insecurity and Health Outcomes,” Health Affairs, 34(11): 1830-1839, 2015, http://gattonweb.uky.edu/Faculty/Ziliak/GZ_HealthAffairs_34(11)_2015.pdf; Daniel Arenas et al., “Negative Health Outcomes Associated with Food Insecurity Status in the United States of America: a Systematic Review of Peer-Reviewed Studies,” September 2018, https://osf.io/preprints/nutrixiv/uk9xw/; and Lesley Weaver and Connor Fasel, “A Systematic Review of the Literature on the Relationships Between Chronic Diseases and Food Insecurity,” Food and Nutrition Sciences, 9(5): 519-541, 2018, https://www.scirp.org/html/7-2702276_84666.htm?pagespeed=noscript.
[12] Alisha Coleman-Jensen, William McFall, and Mark Nord, “Food Insecurity in Households with Children,” Economic Research Service, USDA, May 2013, https://www.ers.usda.gov/webdocs/publications/43763/37672_eib-113.pdf?v=41424; Klébya de Oliveira et al., “Household Food Insecurity and Early Childhood Development: Systematic Review and Meta‐Analysis,” Maternal & Child Nutrition, 16(3): e12967, 2020, https://onlinelibrary.wiley.com/doi/full/10.1111/mcn.12967; and Shannon Simonovich et al., “A Systematic Review Examining the Relationship Between Food Insecurity and Early Childhood Physiological Health Outcomes,” Translational Behavioral Medicine, 10(5): 1086-1097, 2020, https://academic.oup.com/tbm/article-abstract/10/5/1086/5921050.
[13] Jason Nagata et al., “Food Insecurity and Chronic Disease in US Young Adults: Findings from the National Longitudinal Study of Adolescent to Adult Health,” Journal of General Internal Medicine, 34(12): 2756-2762, 2019, https://link.springer.com/article/10.1007/s11606-019-05317-8.
[14] Laraia, op. cit.; Gundersen and Ziliak, op. cit.; and Jennifer Te Vazquez et al., “Food Insecurity and Cardiometabolic Conditions: A Review of Recent Research,” Current Nutrition Reports, 10: 243-254, 2021, https://link.springer.com/article/10.1007/s13668-021-00364-2.
[15] Laraia, op. cit; Gundersen and Ziliak, op. cit.
[16] John T. Cook et al., “Are Food Insecurity’s Health Impacts Underestimated in the U.S. Population? Marginal Food Security Also Predicts Adverse Health Outcomes in Young U.S. Children and Mothers,” Advances in Nutrition: An International Review Journal, 4(1): 51-61, 2013, http://advances.nutrition.org/content/4/1/51.long; and Kayoung Lee, “Household Marginal Food Security Is Associated with Poorer Self-Rated Health in Korean Adults,” Nutrition Research, 10: 33-41, 2022, https://www.sciencedirect.com/science/article/abs/pii/S0271531722000021.
[17] Daphne Hernandez and Alison Jacknowitz, “Transient, but Not Persistent, Adult Food Insecurity Influences Toddler Development,” Journal of Nutrition, 139(8): 1517-1524, 2009, https://academic.oup.com/jn/article/139/8/1517/4670506?login=false; and Rachel Kimbro and Justin Denney, “Transitions Into Food Insecurity Associated with Behavioral Problems and Worse Overall Health Among Children,” Health Affairs, 34(11): 1949-1955, 2015, https://www.healthaffairs.org/action/showCitFormats?doi=10.1377%2Fhlthaff.2015.0626.
[18] Christian A. Gregory and Alisha Coleman-Jensen, “Food Insecurity, Chronic Disease, and Health Among Working-Age Adults,” Economic Research Service, USDA, July 2017, https://www.ers.usda.gov/webdocs/publications/84467/err-235.pdf?v=42942.
[19] Alisha Coleman-Jensen et al., “Household Food Security in the United States in 2021,” Economic Research Service, USDA, September 2022, https://www.ers.usda.gov/publications/pub-details/?pubid=104655. Note that household race and ethnicity is based on the race and ethnicity reported by the household reference person (in whose name the housing unit is owned or rented).
[20] Margaret Thomas, Daniel Miller, and Taryn Morrissey, “Food Insecurity and Child Health,” Pediatrics, 144(4): 2019, https://www.publications.aap.org/pediatrics/article-split/144/4/e20190397/38475/Food-Insecurity-and-Child-Health; and Craig Gundersen and Brent Kreider, “Bounding the Effects of Food Insecurity on Children’s Health Outcomes,” Journal of Health Economics, 28(5): 971-983, (2009), https://www.sciencedirect.com/science/article/abs/pii/S0167629609000708.
[21] Dena Herman et al., “Food Insecurity and Cost-Related Medication Underuse Among Nonelderly Adults in a Nationally Representative Sample,” American Journal of Public Health, 105(10): e48-e59, October 2015, http://ajph.aphapublications.org/doi/full/10.2105/AJPH.2015.302712.
[22] See, for example, Seth A. Berkowitz, Hilary K. Seligman, and Niteesh K. Choudhry, “Treat or Eat: Food Insecurity, Cost-Related Medication Underuse, and Unmet Needs,” American Journal of Medicine, 127(4): 303-310, 2014, http://www.amjmed.com/article/S0002-9343(14)00030-8/fulltext; Chadwick K. Knight et al., “Household food insecurity and medication ‘scrimping’ among US adults with diabetes,” Preventive Medicine, 83: 41-45, February 2016, http://www.sciencedirect.com/science/article/pii/S0091743515003679; Minal R. Patel et al., “Social determinants of health, cost-related nonadherence, and cost-reducing behaviors among adults with diabetes: findings from the National Health Interview Survey,” Medical Care, 54(8): 796-803, August 2016, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4945373/; Patience Afulani et al., “Food Insecurity and Health Outcomes Among Older Adults: The Role of Cost-Related Medication Underuse,” Journal of Nutrition in Gerontology and Geriatrics, 34(3): 319-342, August 12, 2015, http://www.tandfonline.com/doi/abs/10.1080/21551197.2015.1054575; and Brittany Imel and Heather McClintock, "Food Security and Medication Adherence in Young and Middle-Aged Adults with Diabetes," Behavioral Medicine, published online October 25, 2021, https://www.tandfonline.com/doi/abs/10.1080/08964289.2021.1987855.
[23] Herman et al. Researchers found an even steeper gradient among Canadian adults under a different system of health care insurance and prescription drug coverage. After adjusting for differences in socio-demographic characteristics, adults from marginally, moderately, and severely food-insecure households were nearly twice, nearly four times, and about five times more likely, respectively, to delay or not fill prescriptions and skip or reduce doses relative to their food-secure counterparts. See Fei Men et al., “Prescription Medication Nonadherence Associated with Food Insecurity: A Population-Based Cross-Sectional Study,” Canadian Medical Association Open Access Journal, 7(3): E590-E597, 2019 https://www.cmajopen.ca/content/cmajo/7/3/E590.full.pdf.
[24] Zhiwen Xie et al., “Racial and Ethnic Disparities in Medication Adherence Among Privately Insured Patients in the United States,” PLoS One, 14(2): e0212117, 2019, https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0212117.
[25] Though fraught with uncertainty, estimates of the annual economic cost of poor health, illness, and health care associated with food insecurity in the United States range from over $40 billion to as much as $160 billion. See Donald S. Shepard, Elizabeth Setren, and Donna Cooper, “Hunger in America: Suffering We All Pay For,” Center for American Progress, October 2011, https://www.americanprogress.org/article/hunger-in-america/; John T. Cook and Ana Paula Poblacion, “Estimating the Health-Related Costs of Food Insecurity and Hunger,” in The Nourishing Effect: Ending Hunger, Improving Health, Reducing Inequality, Bread for the World, 2016, http://childrenshealthwatch.org/wp-content/uploads/JohnCook_cost_of_hunger_study.pdf, and Seth Berkowitz et al., “State-Level and County-Level Estimates of Health Care Costs Associated with Food Insecurity,” Preventing Chronic Disease, 16(E90), 2019, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6741857/pdf/PCD-16-E90.pdf.
[26] Valerie Tarasuk et al., “Association Between Household Food Insecurity and Annual Health Care Costs,” Canadian Medical Association Journal, 187(14): E429-E436, October 6, 2015, http://www.cmaj.ca/content/187/14/E429. Note that the Canadian classifications (marginal, moderate, and severe) differ from those used to monitor food security in the United States (food insecure and very low food security), though both measures are based on the same set of questions. The authors also report results that include prescription drug benefits. Because these benefits are available only to low-income households in Ontario, and having low income is a strong predictor of food insecurity, their inclusion is likely to confound (and probably overstate) the association between food insecurity and health care costs. As expected, the inclusion of prescription drug costs results in even greater differences in total health care expenditures: 49 percent higher for households with moderate food insecurity and 121 percent higher for those with severe food insecurity.
[27] Fei Men et al., “Food Insecurity Is Associated with Higher Health Care Use and Costs Among Canadian Adults,” Health Affairs, 39(8): 1377-1385, 2020, https://www.healthaffairs.org/doi/abs/10.1377/hlthaff.2019.01637.
[28] Seth A. Berkowitz et al., “Food Insecurity and Health Care Expenditures in the United States, 2011-2013,” Health Services Research, 53(3): 1600-1620, 2018, http://onlinelibrary.wiley.com/doi/10.1111/1475-6773.12730/full. Subsequent research suggests that higher health care spending varies substantially across states and counties, primarily because of differences in the number of food-insecure adults. Per capita spending based on each state’s entire population, not just those who are food insecure, ranges from a high of $243 in Mississippi to a low of $78 in North Dakota. See Berkowitz et al., 2019, op. cit.
[29] Tiffany Fitzpatrick et al., “Looking Beyond Income and Education: Socioeconomic Status Gradients Among Future High-Cost Users of Health Care,” American Journal of Preventive Medicine, 49(2): 161-171, 2015, https://www.sciencedirect.com/science/article/pii/S0749379715000823.
[30] A study using a more nuanced categorization of food security and contemporaneous measures of food security and medical expenditures generally aligns with the conclusion that the use and cost of health care increase as household food insecurity increases. When controls for chronic health conditions are incorporated, however, the differences across food security groups largely dissipate, suggesting that underlying differences in health status may be an important factor in the relationship between food insecurity and health care costs. See Emma Boswell Dean, Michael French, and Karoline Mortensen, “Food Insecurity, Health Care Utilization, and Health Care Expenditures,” Health Services Research, 55(Suppl.2): 883-893, 2020, https://onlinelibrary.wiley.com/doi/pdfdirect/10.1111/1475-6773.13283.
[31] Karl Johnson et al., “Examining the Bidirectional Relationship Between Food Insecurity and Healthcare Spending,” Health Services Research, 56(5): 864-873, 2021, https://onlinelibrary.wiley.com/doi/full/10.1111/1475-6773.13641. It is worth noting that this study determined food security status only once based on a household’s food-related problems in the 30 days before the survey interview took place. Food security, however, can change from month to month as a family’s circumstances improve or worsen. As a result, the question of whether, and how much, the duration of exposure to food insecurity matters for subsequent health care expenditures remains unanswered.
[32] Christine Ma, Lauren Gee, and Margot Kushel, “Associations Between Housing Instability and Food Insecurity with Health Care Access in Low-Income Children,” Ambulatory Pediatrics, 8(1): 50-57, 2008, https://www.sciencedirect.com/science/article/abs/pii/S1530156707001554; and Alon Peltz and Arvin Garg, “Food Insecurity and Health Care Use,” Pediatrics, 144(4): e20190347, 2019, https://publications.aap.org/pediatrics/article/144/4/e20190347/76973/Food-Insecurity-and-Health-Care-Use.
[33] Seth Berkowitz et al., “Food Insecurity, Healthcare Utilization and High Cost: A Longitudinal Cohort Study,” American Journal of Managed Care, 24(9): 399-404, 2018, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6426124/pdf/nihms-1000556.pdf.
[34] Vibha Bhargava and Jung Sun Lee, “Food Insecurity and Health Care Utilization Among Older Adults in the United States,” Journal of Nutrition in Gerontology and Geriatrics, 35(3):177-192, 2016, http://www.tandfonline.com/doi/abs/10.1080/21551197.2016.1200334; Ariella Spitzer, Marisa Shenk, and James Mabli, “Food Insecurity is Directly Associated with the Use of Health Services for Adverse Health Events among Older Adults,” Journal of Nutrition, 150(12): 3152-3160, 2020, https://doi.org/10.1093/jn/nxaa286.
[35] James Mabli et al., “Measuring the Effect of Supplemental Nutrition Assistance Program (SNAP) Participation on Food Security,” Food and Nutrition Service, USDA, 2013, https://www.fns.usda.gov/measuring-effect-snap-participation-food-security-0. By following families as they enter SNAP, this study avoids two major pitfalls that would otherwise make it difficult to assert that participation is responsible for the improvements in food security. First, it avoids the problems associated with self-selection by using these families as their own controls, comparing their food security status just before entering SNAP to their status six months later (rather than to non-participants). Second, it avoids the problems associated with underreporting of SNAP participation in most surveys by drawing the sample of families directly from the records of local SNAP offices. A subsequent publication by the same research team offers slightly revised but substantively similar estimates of the overall impact of SNAP on food security and very low food insecurity. See James Mabli and Jim Ohls, “Supplemental Nutrition Assistance Program Participation Is Associated with an Increase in Household Food Security in a National Evaluation,” Journal of Nutrition, 145(2): 344-351, 2015, https://academic.oup.com/jn/article/145/2/344/4585732.
[36] Caroline Ratcliffe, Signe-Mary McKernan, and Sisi Zhang, “How Much Does the Supplemental Nutrition Assistance Program Reduce Food Insecurity?” American Journal of Agricultural Economics, 93(4): 1082-1098, July 12, 2011, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4154696/.
[37] Seungyeon Cho, “The Effect of Participation in the Supplemental Nutrition Assistance Program on Food Insecurity of Children in US Immigrant Households,” Journal of Family and Economic Issues, September 20, 2021, https://link.springer.com/article/10.1007/s10834-021-09799-9#citeas.
[38] Partha Deb and Christian Gregory, “Heterogeneous Impacts of the Supplemental Nutrition Assistance Program on Food Insecurity,” Economics Letters, 173: 55-60, 2018, https://www.sciencedirect.com/science/article/abs/pii/S0165176518303896.
[39] The demonstration initially provided a monthly benefit of $60 in the summer of 2012 and then compared the relative effectiveness of a smaller benefit ($30) in the summers of 2013 and 2014. The results suggested that both increases produced similar improvements in the most severe form of food insecurity among children. See Ann Collins et al., “Summer Electronic Benefits Transfer for Children (SEBTC) Demonstration: Summary Report,” prepared for the Food and Nutrition Service, USDA, May 2016, https://fns-prod.azureedge.net/sites/default/files/ops/sebtcfinalreport.pdf.
[40] Mark Nord and Mark Prell, “Food Security Improved Following the 2009 ARRA Increase in SNAP Benefits,” ERR-116, Economic Research Service, USDA, April 2011, https://www.ers.usda.gov/webdocs/publications/44837/7469_err116.pdf?v=41056.
[41] For example, see Andrew Bryant and Lendie Follett, “Hunger Relief: A Natural Experiment from Additional SNAP Benefits During the COVID-19 Pandemic,” The Lancet Regional Health - Americas, 10, June 2022, https://www.sciencedirect.com/science/article/pii/S2667193X22000412.
[42] Lauren Bauer et al., “An Update on the Effect of Pandemic EBT on Measures of Food Hardship,” Brookings Institution Hamilton Project, September 29, 2021, https://www.brookings.edu/research/an-update-on-the-effect-of-pandemic-ebt-on-measures-of-food-hardship/. Food insufficiency is a more severe condition than food insecurity and measures whether a household generally has enough to eat. In this way, food insufficiency is closer in severity to very low food security than to overall food insecurity.
[43] Bryant and Follett, op. cit.
[44] Christian A. Gregory and Partha Deb, “Does SNAP Improve Your Health?” Food Policy, 50: 11-19, 2015, http://www.sciencedirect.com/science/article/pii/S0306919214001419; Daniel Miller and Taryn Morrissey, “SNAP Participation and the Health and Health Care Utilization of Low-Income Adults and Children,” Public Health Nutrition, 24(18): 6543-6554, 2021, https://www.cambridge.org/core/journals/public-health-nutrition/article/snap-participation-and-the-health-and-health-care-utilization-of-lowincome-adults-and-children/F0889E87B0104D151582D0C574EE0577; Vanessa Oddo and James Mabli, “Participation in the Supplemental Nutrition Assistance Program and Psychological Distress,” American Journal of Public Health, 6: e30-e35, June 2015, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4431109/pdf/AJPH.2014.302480.pdf; and Harry Adynski, Todd Schwartz, and Hudson Santos, “Does Participation in Food Benefit Programs Reduce the Risk for Depressive Symptoms?” Journal of the American Psychiatric Nurses Association, January 3, 2021, https://journals.sagepub.com/doi/full/10.1177/1078390320983904.
[45] Katherine M. Joyce et al., “Household Hardships, Public Programs, and Their Associations with the Health and Development of Very Young Children: Insights from Children’s HealthWatch,” Journal of Applied Research on Children: Informing Policy for Children at Risk, 3(1), 2012, http://www.childrenshealthwatch.org/wp-content/uploads/KJ_JARC_2012.pdf; Stephanie Ettinger de Cuba et al., “The SNAP Vaccine: Boosting Children’s Health,” Children’s HealthWatch, February 1, 2012, http://childrenshealthwatch.org/the-snap-vaccine-boosting-childrens-health/; and Stephanie Ettinger de Cuba et al., “SNAP, Young Children’s Health, and Family Food Security and Healthcare Access,” American Journal of Preventive Medicine, 57(4): 525-532, 2019, https://www.researchgate.net/profile/Mariana-Chilton/publication/335916252_SNAP_Young_Children's_Health_and_Family_Food_Security_and_Healthcare_Access/links/5d8371da299bf1996f77762d/SNAP-Young-Childrens-Health-and-Family-Food-Security-and-Healthcare-Access.pdf.
[46] Allison Bovell et al., “Making SNAP Work for Families Leaving Poverty,” Children’s HealthWatch, November 2014, http://www.childrenshealthwatch.org/wp-content/uploads/FINALPhilly-Food-to-web3.pdf; and Stephanie Ettinger de Cuba et al., “Punishing Hard Work: The Unintended Consequences of Cutting SNAP Benefits,” Children’s HealthWatch, December 12, 2013, http://childrenshealthwatch.org/punishing-hard-work-the-unintended-consequences-of-cutting-snap-benefits/.
[47] Katelin Alfaro-Hudak et al., “SNAP and Cardiometabolic Risk in Youth,” Nutrients, 14(13): 2756, 2022, https://www.mdpi.com/2072-6643/14/13/2756.
[48] Tae-Young Pak and GwanSeon Kim, “Food Stamps, Food Insecurity, And Health Outcomes Among Elderly Americans,” Preventive Medicine, 130: 105871, 2020, https://www.sciencedirect.com/science/article/abs/pii/S0091743519303470.
[49] Douglas Almond, Hillary Hoynes, and Diane Schanzenbach, “Inside the War on Poverty: The Impact of Food Stamps on Birth Outcomes,” Review of Economics and Statistics, 93(2), May 2011, https://www.mitpressjournals.org/doi/pdfplus/10.1162/REST_a_00089; Hilary Hoynes and Diane Whitmore Schanzenbach, and Douglas Almond, “Long-Run Impacts of Childhood Access to the Safety Net,” American Economic Review, 106(4): 903-934, April 2016, https://pdfs.semanticscholar.org/c94b/26c57bb565b566913d2af161e555edeb7f21.pdf. (It is important to note that much has changed since the initial introduction of the Food Stamp Program, including the introduction and growth of the Special Supplemental Nutrition Program for Women, Infants, and Children, and Medicaid.) An unpublished paper using a similar research approach found mixed results that indicate small or non-existent overall effects of access to food stamps on mortality rates. See Jordan Jones, Charles Courtemanche, and James Marton, “The Impacts of the Food Stamp Program on Mortality,” prepared for presentation at the 2018 Agricultural & Applied Economics Association Annual Meeting, August 2018, https://ageconsearch.umn.edu/record/273845?ln=en..
[50] Angela Fertig, “The Long-Term Health Consequences of Childhood Food Insecurity,” University of Kentucky Center for Poverty Research Discussion Paper 2019-03, May 2019, https://ukcpr.org/sites/ukcpr/files/research-pdfs/DP2019-03.pdf.
[51] Chloe East, “The Effect of Food Stamps on Children’s Health: Evidence from Immigrants’ Changing Eligibility,” Journal of Human Resources, 55(2): 387-427, 2020, http://jhr.uwpress.org/content/55/2/387.
[52] Irma Arteaga, Leslie Hodges, and Colleen Heflin, “Giving Kids a Boost: The Positive Relationship Between Frequency of SNAP Participation and Infant's Preventative Health Care Utilization," SSM-Population Health, 15: 100910, 2021, https://www.sciencedirect.com/science/article/pii/S2352827321001853#bib45.
[53] Hilary Hoynes, Erin Bronchetti, and Garret Christensen, “The Real Value of SNAP Benefits and Health Outcomes,” University of Kentucky Center for Poverty Research, Discussion Paper Series, DP2017-03, January 2017, https://uknowledge.uky.edu/cgi/viewcontent.cgi?referer=&httpsredir=1&article=1104&context=ukcpr_papers; and Erin Bronchetti, Garret Christensen, and Hilary Hoynes, “Local Food Prices, SNAP Purchasing Power, and Child Health,” Journal of Health Economics, 68: 102231, 2019, https://www.sciencedirect.com/science/article/abs/pii/S0167629619304151.
[54] Conversely, some low-income people may spend less on basic needs (such as food, clothing, housing, and transportation) to afford their medications. Research focusing on such individuals who choose medication over basic needs is limited. A study of a small number of low-income adults in St. Louis, Missouri, found that those eligible for or receiving SNAP were somewhat less likely to spend less on basic needs to pay for medication though the difference was not statistically significant. See Karthik Rohatgi et al., “Medication Adherence and Characteristics of Patients Who Spend Less on Basic Needs to Afford Medications,” Journal of the American Board of Family Medicine, 34(3): 561-570, 2021, https://www.jabfm.org/content/jabfp/34/3/561.full.pdf.
[55] Among older SNAP participants in Missouri, for example, about 69 percent were diagnosed with hypertension and 40 percent were diagnosed with diabetes. See Colleen Heflin et al., “Hypertension, Diabetes and Medication Adherence among the Older Supplemental Nutritional Assistance Program Population,” Journal of Applied Gerontology, June 17, 2021, https://journals.sagepub.com/doi/abs/10.1177/07334648211022493.
[56] Mithuna Srinivasan and Jennifer A. Pooler, “Cost-Related Medication Nonadherence for Older Adults Participating in SNAP, 2013–2015,” American Journal of Public Health, 108(2): 224-230, 2018, http://ajph.aphapublications.org/doi/10.2105/AJPH.2017.304176; Jennifer Pooler and Mithuna Srinivasan, “Association Between Supplemental Nutrition Assistance Program Participation and Cost-Related Medication Nonadherence Among Older Adults with Diabetes,” JAMA Internal Medicine, 179(1): 63-70, 2019, https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/2715159.
[57] See Sarah L. Szanton et al., “Food assistance is associated with decreased nursing home admissions for Maryland’s Dually Eligible Older Adults,” BMC Geriatrics, 17(1), 162, 2017, https://bmcgeriatr.biomedcentral.com/articles/10.1186/s12877-017-0553-x; and Laura J. Samuel et al., “Does the Supplemental Nutrition Assistance Program Affect Hospital Utilization Among Older Adults? The Case of Maryland,” Population Health Management, 21(2): 88-95, 2018, https://www.liebertpub.com/doi/full/10.1089/pop.2017.0055. In addition to controlling for demographic and socioeconomic factors that may contribute to differences between SNAP participants and non-participants, hospitalization findings include a control for proportion of time spent on Medicaid. As the authors note, SNAP participants are more likely to participate in Medicaid, and Medicaid participation is linked with hospital utilization. Models that do not include this control (but do control for demographic and socioeconomic factors) find that SNAP participants had a 14 percent lower probability of hospitalization compared to non-participants.
[58] Seth Berkowitz et al., “Supplemental Nutrition Assistance Program Participation and Health Care Use in Older Adults: A Cohort Study,” Annals of Internal Medicine, 174(12): 1674-1682, 2021, https://www.acpjournals.org/doi/abs/10.7326/M21-1588.
[59] Chinedum Ojinnaka and Colleen Heflin, “Supplemental Nutrition Assistance Program Size and Timing and Hypertension-Related Emergency Department Claims Among Medicaid Enrollees,” Journal of the American Society of Hypertension, 12(11): e27-e34, 2018, https://www.sciencedirect.com/science/article/abs/pii/S1933171118302869.
[60] Chloe East and Andrew Friedson, “An Apple A Day? Adult Food Stamp Eligibility and Health-Care Utilization among Immigrants,” American Journal of Health Economics, 6(3): 289-323, 2020, https://research.upjohn.org/cgi/viewcontent.cgi?article=1313&context=up_workingpapers. As noted above, the changes in immigrant eligibility due to the 1996 law that changed basic needs programs and subsequent legislation allow for a relatively strong test of the impact of SNAP on health care utilization and outcomes.
[61] J. Kim, “Are Older Adults Who Participate in the Supplemental Nutrition Assistance Program Healthier Than Eligible Nonparticipants? Evidence from the Health and Retirement Study,” Gerontologist, 55 (Supplement Issue 2): 672, November 1, 2015, https://academic.oup.com/gerontologist/article/55/Suppl_2/672/2489236.
[62] A study focused on children found that those who participated consistently in SNAP over the course of two years had lower unadjusted health care expenditures compared to children who did not participate, but these differences were not significant after controlling for characteristics of the child, parent, and household. It is possible that longer time horizons, likely well beyond 24 months, are needed to detect the effects that programs which moderate food insecurity among children have on health care expenditures. See Stephen Rogers et al., "Supplemental Nutrition Assistance Program Participation and Health Care Expenditures in Children," BMC Pediatrics, 22(155), 2022, https://link.springer.com/article/10.1186/s12887-022-03188-3.
[63] Seth A. Berkowitz et al., “Supplemental Nutrition Assistance Program (SNAP) Participation and Health Care Expenditures Among Low-Income Adults,” JAMA Internal Medicine, November 2017, https://jamanetwork.com/journals/jamainternalmedicine/article-abstract/2653910?amp%3butm_source=JAMA+Intern+MedPublishAheadofPrint&utm_campaign=25-09-2017; and Seth Berkowitz, Hilary K. Seligman, and Sanjay Basu, “Impact of Food Insecurity and SNAP Participation on Healthcare Utilization and Expenditures,” University of Kentucky Center for Poverty Research Discussion Paper Series, DP2017-02, 2017, http://uknowledge.uky.edu/cgi/viewcontent.cgi?article=1105&context=ukcpr_papers. An older study that did not fully account for unobserved differences did not find a significant difference in Medicare spending among low-income elderly with diabetes between those who received food stamps (as SNAP was known then) and those who did not.
[64] See Lauren H. Nicholas, “Can Food Stamps Help to Reduce Medicare Spending on Diabetes?” Economics and Human Biology, 9(1): 1-13, January 2011, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3032985/. Still older work using a different data set and analytic approach concluded that SNAP increased medical expenses of non-elderly women by $300 to $700 per year, mainly because program benefits freed up additional discretionary income that could be spent on medical care. See Chad D. Meyerhoefer and Yuriy Pylypchuk, “Does Participation in the Food Stamp Program Increase the Prevalence of Obesity and Health Care Spending?” American Journal of Agricultural Economics, 90(2): 287-305, May 1, 2008, https://onlinelibrary.wiley.com/doi/10.1111/j.1467-8276.2007.01125.x.
[65] Some enrollment groups, such as adults who gained eligibility through Affordable Care Act Medicaid expansions, receive federal match rates outside of this range.
[66] While states are responsible for half of the administrative cost of eligibility determinations, employment and training, nutrition education, and anti-fraud activities, these costs represent a small part of SNAP’s overall costs. In fiscal year 2021, the federal government spent about $114 billion on SNAP, including emergency relief funding in response to the COVID-19 pandemic. Ninety-five percent went directly to benefits that households used to purchase food, and less than 4 percent went to state administrative costs.
[67] Joseph Llobrera, Matt Saenz, and Lauren Hall, “USDA Announces Important SNAP Benefit Modernization,” Center on Budget and Policy Priorities, August 26, 2021, https://www.cbpp.org/research/food-assistance/usda-announces-important-snap-benefit-modernization.
[68] Mark Nord and Mark Prell, “Food Security Improved Following the 2009 ARRA Increase in SNAP Benefits,” Economic Research Service, USDA, April 2011, https://www.ers.usda.gov/publications/pub-details/?pubid=44839; Jiyoon Kim, “Do SNAP Participants Expand Non-Food Spending When They Receive More SNAP Benefits? — Evidence from the 2009 SNAP Benefits Increase,” Food Policy, 65: 9-20. 2016, https://www.sciencedirect.com/science/article/abs/pii/S0306919216304341.
[69] Taryn Morrissey and Daniel Miller, “Supplemental Nutrition Assistance Program Participation Improves Children’s Health Care Use: An Analysis of the American Recovery and Reinvestment Act's Natural Experiment,” Academic Pediatrics, 20(6): 863-870, 2020, https://www.sciencedirect.com/science/article/abs/pii/S1876285919304619.
[70] Katelin Hudak, Elizabeth Racine, and Lisa Schulkind, “An Increase in SNAP Benefits Did Not Impact Food Security or Diet Quality in Youth,” Journal of the Academy of Nutrition and Dietetics. 121(3): 507-519, 2020, https://www.sciencedirect.com/science/article/abs/pii/S2212267220313198.
[71] Laura Samuel et al., “Supplemental Nutrition Assistance Program 2009 Expansion and Cardiometabolic Markers among Low-Income Adults,” Preventive Medicine, 150: 106678, 2021, https://www.sciencedirect.com/science/article/abs/pii/S0091743521002474.
[72] Rajan Sonik, “Massachusetts Inpatient Medicaid Cost Response to Increased Supplemental Nutrition Assistance Program Benefits,” American Journal of Public Health, 106(3): 443-44, 2016, https://ajph.aphapublications.org/doi/full/10.2105/AJPH.2015.302990; and Rajan Sonik, Susan Parish, and Monika Mitra, “Inpatient Medicaid Usage and Expenditure Patterns After Changes in Supplemental Nutrition Assistance Program Benefit Levels,” Preventing Chronic Disease, 15: E120, 2018, https://stacks.cdc.gov/view/cdc/60010.
[73] See Stacy Gleason, Dani Hansen, and Breanna Wakar, “Indicators of diet quality, nutrition, and health for Americans by program participation status: SNAP Report,” Food and Nutrition Service, USDA, December 2021, https://www.fns.usda.gov/snap/indicators-diet-quality-nutrition-and-health-americans-program-participation-status-2011; Chelsea Singleton et al., “Examining disparities in diet quality between SNAP participants and non-participants using Oaxaca-Blinder decomposition analysis,” Preventive Medicine Reports, 19: 101134, 2020, https://www.sciencedirect.com/science/article/pii/S2211335520300942; Yu Chen et al., “Nutritional quality of retail food purchases is not associated with participation in the Supplemental Nutrition Assistance Program for nutrition-oriented households,” Plos One, 15(12): e0240263, 2020, https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0240263; and Fang Zhang et al., “Trends and disparities in diet quality among US adults by Supplemental Nutrition Assistance Program Participation status,” JAMA Network Open, 1(2): e180237, 2018, https://jamanetwork.com/journals/jamanetworkopen/article-abstract/2684625.
[74] See Steven Garasky et al., “Foods typically purchased by Supplemental Nutrition Assistance Program (SNAP) households,” Food and Nutrition Service, USDA, November 2016, https://www.fns.usda.gov/snap/foods-typically-purchased-supplemental-nutrition-assistance-program-snap-household; Anna Grummon and Lindsey Smith Taillie, “Nutritional profile of Supplemental Nutrition Assistance Program household food and beverage purchases,” American Journal of Clinical Nutrition, 105(6): 1433-1442, 2017, https://academic.oup.com/ajcn/article/105/6/1433/4633995; Gleason, Hansen, and Wakar, op. cit; and Marilyn Tseng et al., “Fruit and Vegetable Purchasing Patterns and Supplemental Nutrition Assistance Program Participation: Findings From a Nationally Representative Survey,” Journal of the Academy of Nutrition and Dietetics, 120(10): 1633-1642, 2020, https://www.sciencedirect.com/science/article/pii/S2212267220305165.
[75] See Mary Kay Fox, William Hamilton, and Biing-Hwan Lin (eds.), “Effects of Food Assistance and Nutrition Programs on Nutrition and Health: Volume 3, Literature Review,” Economic Research Service, USDA, 2004, https://www.ers.usda.gov/webdocs/publications/46556/30240_fanrr19-3_002.pdf?v=0 ; IOM (Institute of Medicine) and NRC (National Research Council), “Supplemental Nutrition Assistance Program: Examining the Evidence to Define Benefit Adequacy, 2013, https://pubmed.ncbi.nlm.nih.gov/23858096/; Tatiana Andreyeva, Amanda Tripp, and Marlene Schwartz, “Dietary Quality of Americans by Supplemental Nutrition Assistance Program Participation Status: A Systematic Review,” American Journal of Preventive Medicine, 49(4): 594-604, 2015, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6022372/; and Prageet Sachdev, Mahsa Babaei, and Jeanne Freeland-Graves, “Supplemental Nutrition Assistance Program (SNAP): does receiving assistance impact food choices?” Nutrition and Dietary Supplements, 11: 19-35, 2019, https://www.proquest.com/openview/34b4a3e3e255d405728b6e51449c7107/1?pq-origsite=gscholar&cbl=3933339.
[76] Geetha Waehrer, Partha Deb, and Sandra L. Decker, “Did the 2009 American Recovery and Reinvestment Act affect dietary intake of low-income individuals?” Economics & Human Biology, 19: 170-183, 2015, https://www.sciencedirect.com/science/article/pii/S1570677X1500060X; and Hudak, Racine, and Schulkind, op. cit.
[77] Michele Ver Ploeg and Chen Zhen, “Changes in SNAP Benefit Levels and Food Spending and Diet Quality: Simulations from the National Household Food Acquisition and Purchase Survey,” Center on Budget and Policy Priorities, May 12, 2022, https://www.cbpp.org/research/food-assistance/changes-in-snap-benefit-levels-and-food-spending-and-diet-quality.
[78] Marianne P. Bitler, “The Health and Nutrition Effects of SNAP: Selection into the Program and a Review of the Literature on Its Effects,” in SNAP Matters: How Food Stamps Affect Health and Well-Being, 2016, http://www.ukcpr.org/sites/www.ukcpr.org/files/documents/DP2014-02_0.pdf; Gregory and Deb (2015); and Zach Conrad, Colin D. Rehm, Parke Wilde, and Dariush Mozaffarian, “Cardiometabolic Mortality by Supplemental Nutrition Assistance Program Participation and Eligibility in the United States,” American Journal of Public Health, 107(3): 466-474, March 2017, https://www.ncbi.nlm.nih.gov/pubmed/28103061.
[79] Charles Courtemanche, Augustine Denteh, and Rusty Tchernis, “Estimating the Associations Between SNAP and Food Insecurity, Obesity, and Food Purchases with Imperfect Administrative Measures of Participation,” Southern Economic Journal, 86(1): 202-228, 2019, https://www.nber.org/system/files/working_papers/w24412/w24412.pdf. Although this paper assesses the associations between SNAP participation and food security, obesity, and diet quality, it does so without accounting for self-selection into the program as this was outside the scope of the project. The results are best interpreted as indications of negative selection, that those with greatest need (that is, more food insecure and less healthy) are more likely to participate than others.
[80] An exception in the literature is Brent Kreider et al., “Identifying the Effects of SNAP (Food Stamps) on Child Health Outcomes When Participation Is Endogenous and Misreported,” Journal of the American Statistical Association, 107(499): 958-975, September 2012, http://batten.virginia.edu/sites/default/files/research/attachments/JASA_KPGJ_online(1).pdf. Using relatively strong but plausible assumptions to address self-selection and classification errors simultaneously, the authors estimate that SNAP reduces the prevalence of child food insecurity by at least 8 percentage points.
Más de los autores

Steven Carlson is a research analyst who previously directed the Office of Policy Support at the Agriculture Department’s Food and Nutrition Service.
